

Diana Mikula, the executive director of the Mississippi Department of Mental Health, said the state’s mental-health system is moving in the right direction—but not fast enough to avoid a lawsuit from the U.S. Department of Justice. Photo by Imani Khayyam.
JACKSON — The mood shift in the old Mississippi Supreme Court room was palpable last week when the Department of Mental Health faced a group of legislators tasked with evaluating the agency's effectiveness and expenditures in upcoming months.
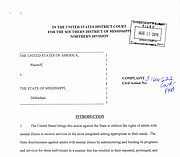
That's because the elephant in the room would not stay quiet: The U.S. Department of Justice has sued the State of Mississippi for failing to provide enough community-based services to individuals with mental illnesses and developmental disabilities, by over-relying on institutionalization.
What baffled lawmakers was exactly why the State still managed to get sued after appropriating additional monies to the department (like increasing funding by $16.1 million each year since fiscal-year 2015) to increase the state's offerings in community-based mental-health services.
Starting in 2008, the State began closing beds in the state psychiatric hospitals—close to 500—by not replacing patients' spots after they were discharged, lawmakers recalled last week. This was before the DOJ even got involved in Mississippi's mental health-care system. But by 2011, the State was still struggling to provide enough community-based services, and consequently, several mentally ill Mississippians began to cycle in and out of state hospitals. One 27-year-old man at Mississippi State Hospital in March 2015 had 22 prior admissions to the hospital, the Aug. 11 DOJ complaint says.
The DOJ made the State publicly aware of its compliance issues with the Americans with Disabilities Act and the Olmstead U.S. Supreme Court ruling, which supports community-based services for those with mental illnesses under ADA, in 2011 when then-Gov. Haley Barbour received a findings letter that said Mississippi has "the most institution-reliant system in the United States."
A September 2015 progress update report from the Department of Mental Health says that "the Attorney General and Jonathan Smith, chief of the Special Litigation Section for DOJ, signed a letter outlining the next steps for...settling these alleged Olmstead/ADA violations." The same 2014 letter is referenced in a May 12, 2015, PEER report that says that the letter did not constitute an admission to factual allegations from the DOJ on the state's system but instead outlined actions, like the Legislature appropriating more money and expanding waiver options, to ensure more community-based mental healthcare for Mississippians.
Something happened between September and this summer, however, because in his news release following the DOJ's announcement, Jim Hood said his office had been negotiating for several years to avoid litigation.
"The Attorney General refused to accept the federal government's demands for a court-ordered consent decree that would bind the state to perpetual federal oversight," the Aug. 11 press release states.
Other states served with similar letters have entered consent decrees or settlement agreements with the DOJ to avoid litigation, which Hood said in his press release would be "a considerable cost to the state."
What Other States Do
It's not that Mississippi did not react when they received their findings letter in 2011, but other states put in similar circumstances at the time reacted quicker.
Delaware received a letter in 2010, similar to Mississippi's.
"[W]e have concluded that the State's current mental health system fails to provide services to individuals with mental illness in the most integrated setting appropriate to their needs as required by the ADA," the 2010 DOJ letter to Delaware states. "This has resulted in needless prolonged institutionalization of many individuals with disabilities in DPC (Delaware Psychiatric Center) who could be served in the community."
Delaware is a smaller state than Mississippi with a population of around 935,000. DPC is its only state hospital for mentally ill patients, but even in a small state with one hospital, Delaware could have been doing more in 2010 to offer community-based care. The new secretary of the state's Department of Health and Social Services, Rita Landgraf, knew it.
Landgraf came from an advocacy background and knew a lot about the state's problems with mental-health care, so when she received the notice from the U.S. Department of Justice, she wasted no time taking action. The state ended up with a court-sanctioned settlement agreement, signed in 2011, that lasted five years.
Landgraf said she planned on working to change the state's mental-health care system, but said the agreement with DOJ expedited the process and brought the problem to the attention of state lawmakers.
"The settlement agreement gave us an opportunity to transform the system a bit quicker than if we didn't have a settlement agreement," Landgraf told the Jackson Free Press in an interview.
Landgraf and her staff had the support of their governor, as well as the general assembly, to appropriate more funding for the changes that were necessary in order to meet the requirements of the settlement agreement. Part of that support came from Landgraf's ability to educate lawmakers on the importance of evolving the state's system.
"I think in any state that has this level of transformation, you can't do it with the existing funds; it's not going to happen," Landgraf said. "Here's what I would say, though. I had to educate them (lawmakers) not only on the settlement agreement but on that transformation ... (and) the fact that we would invest in the system now and get a good return on investment in the future."
The Delaware Department of Health and Social Services has continued to downsize its psychiatric hospital since 2011, and Landgraf says that DPC has now cut its patient admissions in half. For every one person who receives services in the hospital, three are out in the community receiving services.
"I've been able to downsize as I invest in the community," she said. "I can take my budget that goes to these facilities, along with my community budget, and move some of those fiscal resources in to the community."
It's not a perfect system, however, because some of the funds that go to the hospital are necessary to help keep the building up and functioning. Regardless, it's cheaper to treat individuals with mental illness in the community versus in institutional care.
Mississippi: 'Not Fast Enough'
Diana Mikula, the executive director of DMH, addressed the DOJ lawsuit briefly at the capitol last week, telling lawmakers that even DOJ acknowledges that the state is offering the right types of community-based services, but that "they just want more, and that's what I believe is going to happen."
"We are going to be addressing the need for more waiver spots, the need for more local crisis teams, the need for more PAC teams, community-treatment teams, crisis-stabilization units," Mikula told lawmakers.
She said the state's 14 community mental-health centers are doing an excellent job offering community-based services and that the State, including the Legislature with appropriations, made a good-faith effort in avoiding the litigation.
"They (community mental-health centers) need more money, and it came down to we just didn't do it fast enough," Mikula said.
The Olmstead ruling, as well as a 2003 national commission that then-President George W. Bush put together, both echo what good research on mental-health care says: Individuals with serious mental illnesses can recover with access to treatment in their own communities, not institutions.
The over-reliance on state hospitals is not unique to Mississippi; institutionalization had been the norm in this country until the 1960s, when there was a federal push to move toward community-based services for the mentally ill. States transitioned to behavioral-health treatment, and in Mississippi, behavioral-health programs are run in Mississippi's state hospitals and regional centers.
Four state hospitals and two residential programs make up DMH's behavioral-health programs. The state also offers six centers for people with intellectual and developmental disabilities. Hospitals and residential centers, while necessary for some patients, do not qualify as "community-based services."
More community-based services are available to Mississippians, offered through one of the state's 14 community mental-health centers, as well as through community organizations and nonprofits that run programs and services funded by the DMH.
However, the majority of state funds in the DMH budget in the past years have gone toward keeping state hospitals and regional centers open.
For example, the DMH Central Office Service Budget of the department, which funds the state's 14 community mental-health centers and providers who offer community-based mental-health care services, spent $69.6 million in fiscal year 2016, legislative budget office data shows. The Mississippi State Hospital alone spent $127.6 million of the state's money in the same year.
Landgraf echoed what Mikula told lawmakers last week at the Mississippi Capitol about transformational change in the mental-health care system: It takes time.
"It's an evolving system, even when you transform what you created today to have a really good system of care, in health, that you want it to continue to evolve," Landgraf said. "What happens in government because we are a system, and we're very bureaucratic, sometimes, we can't respond to that level of transformation."
Community mental-health advocate and executive director of Families as Allies Joy Hogge, who attended last week's working group at the capitol, said that not only lawmakers, but consumers also need to be educated in best practices in mental-health care, particularly that institutionalization should be used to stabilize patients who need it, but community-based services should be the go-to service to help both patient and provider.
"People will tell you what they need—that's a wonderful way to start developing services," she told the Jackson Free Press. "We really haven't done that in this state: We don't develop the services, and I don't think people have that information."
Delaware's settlement agreement, five years later, seemed to work; the ninth court monitor's report says "the State is on track to fulfill its overall obligations under the Agreement." Landgraf asked the Delaware general assembly to create a commission to continue to monitor the state's mental-health care system even after the settlement goes away.
The State of Mississippi will now face litigation fees associated with the DOJ lawsuit, and for lawmakers in January, it means another budgetary consideration. As chairman of the House Public Health and Human Services Committee Sam Mims, R-McComb, said last week, "I'm very concerned about how it's (the lawsuit) going to affect (the) appropriation process next session."
Email state reporter Arielle Dreher at arielle@jacksonfreepress.com.
More like this story
- The State of Mental Health in Mississippi
- AG Hood: State Must Fund Mental Health Care, Not Ignore Lawsuit
- Encouraging Mississippians to 'Think Again' About Mental Illness
- Will a Court Force Mississippi to Change on Mental Health?
- Feds Sue Mississippi for Discrimination Against Adults with Mental Illness
More stories by this author
Support our reporting -- Follow the MFP.

Comments
Use the comment form below to begin a discussion about this content.